

Endometriosis
Endometriosis is an inflammatory condition that affects as many as 10-15% of women. It is present in 50% of women with infertility.


This article is part of a 4 part series, click on the hyperlinks to take you to the other chapters
Endometriosis
Endometriosis is an inflammatory condition that affects as many as 10-15% of women6. It is present in 50% of women with infertility1. It may affect any menstruating woman independent of age. It has now been accepted that dysmenorrhea from the menarche may be due to endometriosis, the concept that it occurred only in older women developed as this was the age that surgical confirmation, via laparoscopy, of the condition was usually achieved. Treatment for adolescents is now considered3. The predominant symptom experienced by women with this condition is chronic pelvic pain. This pain may or may not be associated with menstruation with some women experiencing pain over the whole month. The presence of chronic pelvic pain affects a woman’s self-esteem and quality of life 6,7,8 and is associated with increased absenteeism from work and accounts for nearly 60% of total work productivity loss 7. Homœopathy provides effective treatment for this condition which is affordable and non-invasive, without the need for a definitive diagnosis.
Anatomy
The female reproductive system consists of the uterus, fallopian tubes, ovaries and cervix. Under hormonal influences, the endometrial lining of the uterus proliferates to be able to receive a fertilized ovum which embeds in the lining as the first stage of pregnancy. If fertilization has not taken place the uterine lining will shed and exit the body.
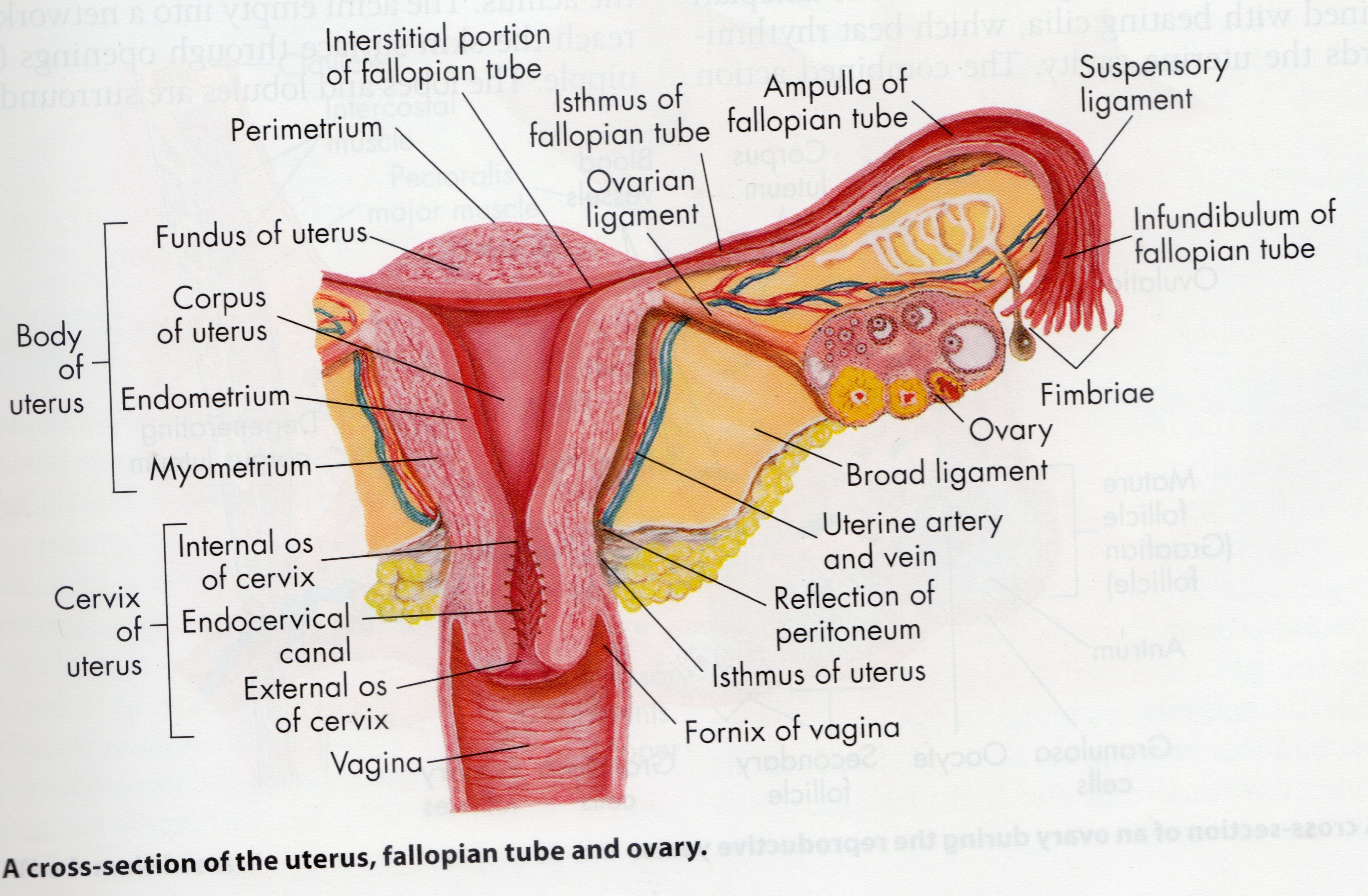
Fig1: Female reproductive system Understanding Pathophysiology; J Craft, C Gordon, A Tiziani and SE Huether, KL McCance, VL Brashers, NS Rote; Mosby Elsevier; 2011; pg 949
Ectopic Sites
In endometriosis some endometrial tissue is found outside the uterus which induces a chronic inflammatory reaction10. The tissue exits through the open ended fallopian tube and can deposit at various sites2 including;
Ovaries
Rectouterine pouch
Outer surface of uterus
Sigmoid colon
Pelvic and abdominal lymph nodes
Cervix
Abdominal wall
Kidneys
Urinary bladder
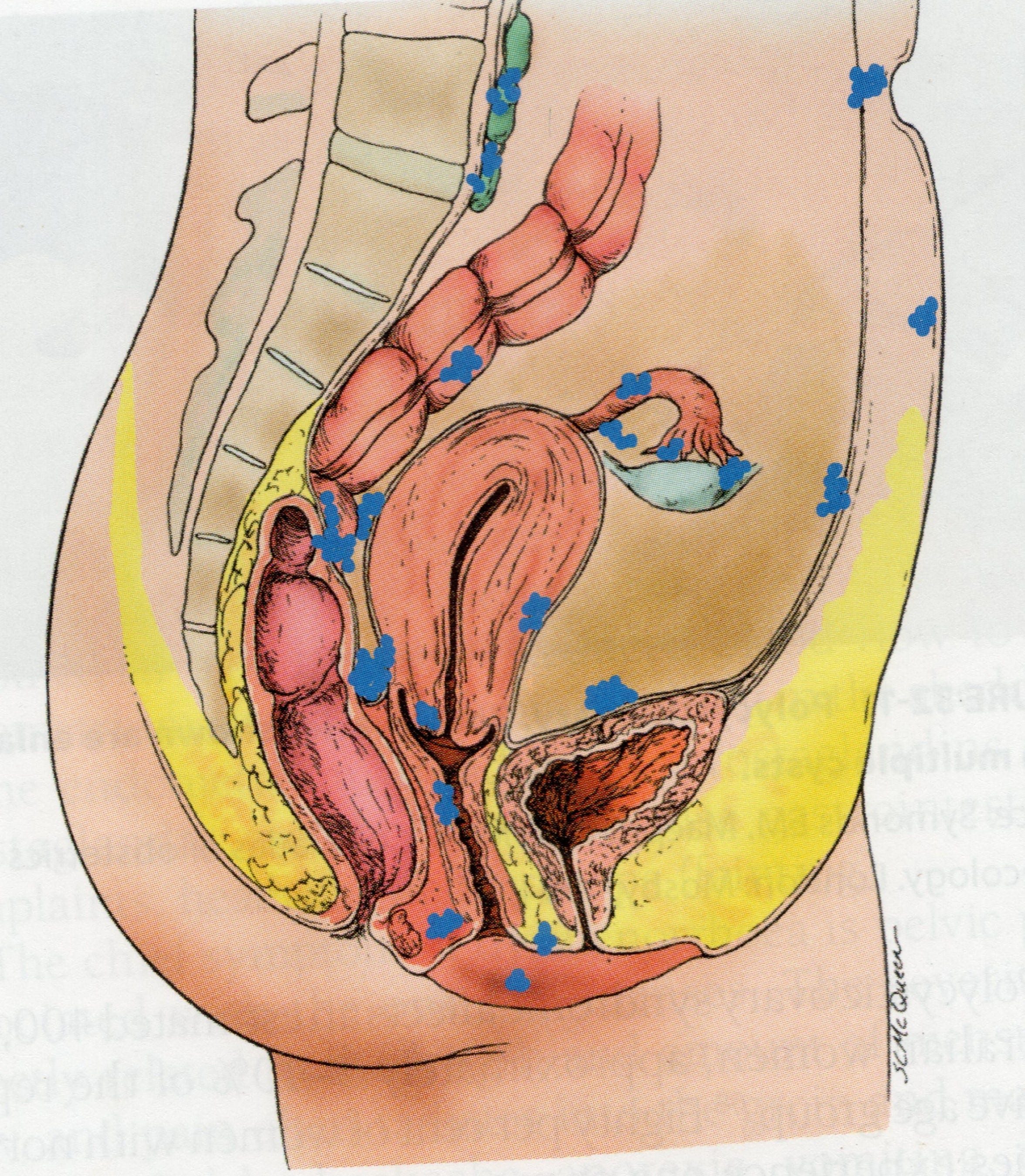
Common sites of endometrial tissue Understanding Pathophysiology; J Craft, C Gordon, A Tiziani and SE Huether, KL McCance, VL Brashers, NS Rote; Mosby Elsevier; 2011; pg 993
The ectopic endometriotic tissue is fundamentally different from eutopic endometrium within the uterus as it produces different cytokines and prostaglandins, synthesizes and metabolizes oestrogen differently and responds to progesterone differently26.
Hormones
There is a closely balanced array of hormones that influence the menstrual cycle and it is these that are manipulated by conventional medicine in an effort to bring about relief. Briefly these are:-
Gonadotropin releasing hormone (GnRH) released from the Hypothalamus.
This stimulates the release of Follicle Stimulating Hormone (FSH) and Luteinising Hormone (LH) from the Anterior Pituitary Gland.
FSH stimulates the ovaries by signaling the initial development of ovarian follicles and their growth.
LH stimulates the growth of follicles and the formation of the corpus luteum, hence triggering ovulation. It also stimulates the follicle to produce androgens
FSH and LH stimulate ovarian follicles to secrete oestrogen.
A rise in oestrogen and/or progesterone provides a feedback loop which then reduces the production of FSH and LH.
Progesterone is produced by the ovaries and functions to prepare the uterine lining for implantation of a fertilized ovum.
Oestrogen is produced by the ovaries and adipose tissue. It functions to develop oocytes, maintain female reproductive structures and other female sex characteristics. It also functions to maintain fluid and electrolyte balance, and protein anabolism. There are 3 main types of oestrogen including β-oestradiol, oestrone and oestriol.
β-oestradiol is the form of oestrogen that induces proliferation and drives inflammation.
Symptoms
The primary symptom of endometriosis is chronic pelvic pain (CPP). Although worldwide statistics show that 1 in 10 women have endometriosis, 1 in 5 suffers from CPP9. Dysmenorrhoea (pain during menstruation) is the primary symptom being present in 50%-90% of women diagnosed8 however there is much more to what could be considered a syndrome.
The pain may manifest as
Severe dysmenorrhoea
Dyspareunia (painful intercourse)
Dyschezia (pelvic pain with defecation)
Chronic pelvic pain (CPP)
Pain on ovulation
Abdominal pain
Concommittant conditions include 6,12,35
Irritable bowel syndrome
Painful bladder syndrome (Interstitial cystitis)
Repetitive kidney stones
Vulvodynia (pain or extreme sensitivity on external genitalia)
Sexual dysfunction and dissatisfaction
Temporomandibular syndrome (pain or dysfunction of TMJ)
Migraine
Fibromyalgia
Chronic fatigue syndrome
Infertility
Depression and anxiety
Symptoms overlap with pelvic inflammatory disease (PID) and a definitive diagnosis is obtained by laparoscopic evaluation. Laparoscopic evaluation is recommended in the ESHRE guidelines as the gold standard in diagnosis.10
Chronic pain is defined as being present for greater than or equal to six (6) months. The type of pain experienced in endometriosis varies and is characteristically associated with the menstrual cycle although it may also be present outside of this time. It may occur before, during or after the menses as well as at ovulation. There may or may not be a clear pattern to the occurrence of pain, it may occur unpredictably and intermittently or be continuous. The pain has differing characteristics that may include dull, throbbing or sharp stabbing, burning pain and hypersensitivity may also be experienced and is associated with neuropathic pains.8 The location may be only in the pelvis or extend to back, legs, etc. All these scenarios are covered in the homeopathic repertory.
Under laparoscopy, the pelvic cavity is described as having a ‘gunshot’ appearance10 due to the colouration of the endometriotic growths on ectopic sites (page 4) These lesions may be black, dark-brown, or bluish puckered lesions, nodules or small cysts containing old haemorrhage surrounded by a variable extent of fibrosis. The dark bluish black colours are considered to be full or diagnostic endometriosis.10,12 Endometriomas are lesions that contain congealed blood and appear with these colours. Other colours may occur, including red, white, pink, yellowish-brown and clear, serous fluid containing vesicles which are considered to be non-classic or subtle lesions12. Endometriomas are sometimes referred to as chocolate cysts and may become as large as a tennis ball, large lesions may create torque of the ovary about the fallopian tube causing severe pain and totally occluding the fallopian tube. In these conditions, surgical removal of the cyst is recommended.
Concomitant symptoms
Infertility may be due to alterations in reproductive anatomy due to growths and scaring. Decreased egg quality, embryo quality and rate of implantation are also found in women with endometriosis. Assisted reproductive technologies are usually offered to overcome these issues. Associated hormonal imbalance such as high oestrogen and low progesterone levels may also influence fertility.
Altered bowel habit is common and presents in a varied manner including diarrhoea alternating with constipation, diarrhoea associated with menses, and undigested food in the stool. IBS is strongly associated with endometriosis.6 This occurs as the same neurological pathways affecting smooth muscle tissues are stimulated. Nausea, distension and early satiety are other digestive symptoms that are associated with the condition and are typically cyclic8.
Fatigue often accompanies chronic pain simply because being in constant pain wears you out! It can become debilitating and lead to chronic fatigue syndrome.
The presence of pain causes associated muscles to become tight which may lead to associated pain in abdomen, thighs, back, neck and headache. Regular massage and/or osteopathic treatment may be beneficial in releasing this tension.
Women’s health-related quality of life (HRQoL) is lower in women experiencing the chronic pain of endometriosis and there is a direct relationship with the amount and intensity of pain and HRQoL6,8. This condition affects not just the physical body but also affects their mental and social wellbeing.
Since the symptoms of endometriosis overlap with other inflammatory conditions, there is often a delay in diagnosis as a laparoscopy must be carried out to determine the condition. This delay may be from 3 to 10 years, and require repeated visits to the doctor before referral to a gynaecologist is granted.7,8
The American Society for Reproductive Medicine has devised a scoring system to determine the staging of the disease with Stage I indicating minimal disease and Stage IV indicating severe disease. However the stage of disease does not correlate with the severity of pain experienced.8
Associated conditions that may either be concurrent with endometriosis or are involved in a differential diagnosis are; pelvic inflammatory disease, pelvic adhesions, ovarian cysts, ovarian masses, leiomyomata, adenomyosis; irritable bowel syndrome, inflammatory bowel disease, interstitial cystitis (painful bladder syndrome), myofascial pain, depression and a history of sexual abuse8.
A history of medical drugging with repeat courses of antibiotics, hormonal manipulation with synthetic hormones and habitual use of pain killing medications also contribute to endocrine imbalance and the overall health of the woman.33,43
This is taken from my thesis written in 2016. References are available on request. Next post will cover the pathophysiology of endometriosis.